
USAID

The challenge
The shortage of medical staff and medical centers has open the doors for innovative models of care, in 2007 Facility-based ART adherence cubs were pilot as a way to decongest medical facilities by shifting consultations and ART collections for stable patients to adherence clubs in the community.
Adherence clubs were found to be an effective model. The improved outcomes in the adherence clubs were determined to be the result of shorter waiting times, higher acceptability of services and consequently fewer missed clinic appointments. A costeffectiveness study showed the cost per patient year was US$58 in the ART club model, vs. US$109 in the mainstream model of care. This model was taken up by the City of Cape Town and Western Cape health services in 2011 and by June 2013, 776 adherence clubs have been implemented and more are on their way in every community.One of the main challenges was the registration of patients, monitoring provision of services and medicines. The other challenge was keeping track of patient data and creating reports to assess the feasibility of such roll-outs as well as the conditions that need to be in place for these models to succeed. There was a need for simplification and technology, but medical software systems are just too expensive and difficult to learn
Innovative models of care require an innovative model of data tracking
In June 2014 EngageBuilder was used as a pilot project to enroll patients and track provision of services by adherence clubs. Tablets and our mobile survey platform are used to enroll and track service provision. This worked but combining the enrollment data with the other survey data to create a patient record with historical data was quite of bit of work. And finding qualify technical staff to make sense of the data was even more challenging and did not provide real-time business intelligence (BI) in order to make informed decisions.
With this in mind we proposed a tracking patient system, they agree and we started to developed it, at this point we did not wanted to disrupt what was in place so we decided to make a module that would combine survey data and make it dynamic and historical. The end result was EB-Dynamics.
How it works
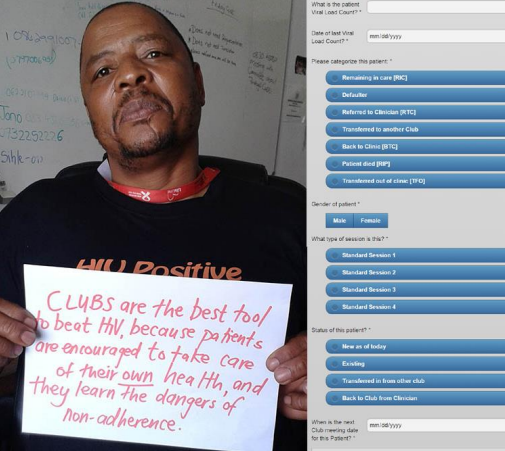
By using EngageBuilder mobile surveys non-clinical staff enrolls patients into the adherence club just by filling in a few questions and pressing buttons on the screen. Once enrolled a second survey (call provision) is used to record and monitor patient’s CD4, viral count, weight and provision of medicines. The data is recorded under the survey database and seamlessly passed to EBDynamics where the patient record can be track, edited and change patient status.

ll numeric fields Weight, CD4 and viral count are reported by patient and provide a full view of the health of the patient over time.
Patient are schedule every two months, weight, CD4, and viral count are recorded using EngageBuilder surveys and historical data is updated in real-time into EB-Dynamics for reporting.
EngageBuilder and EB-dynamics makes it simple and provide real-time reports to measures patient history as well as the success of each adherence club in the community.
Conclusion
EB-Dynamics is helping adherence clubs in South Africa by making data accessible in realtime to better understand and help their effectiveness in the community. This project has been so successful that other adherence clubs in South Africa and nearby countries like Lesotho and Swaziland are looking to purchase our platforms.






